Three GLP-receptor agonists now dominate the metabolic research compound market: semaglutide, tirzepatide, and retatrutide. They are related but not interchangeable. Each targets a different combination of receptors, carries different structural complexity, and presents different procurement challenges in 2026. Researchers choosing between them need to understand the mechanism differences first, then the supply-chain realities second. This article covers both, with notes from COA audits we have run across all three compounds.
One clarification upfront: this is a research-framing comparison. None of these compounds is approved for unsupervised use as a medicine. All three are supplied under Research Use Only (RUO) designation, and everything below reflects in-vitro and preclinical research context only.
Receptor Targets: Where the Three Compounds Differ
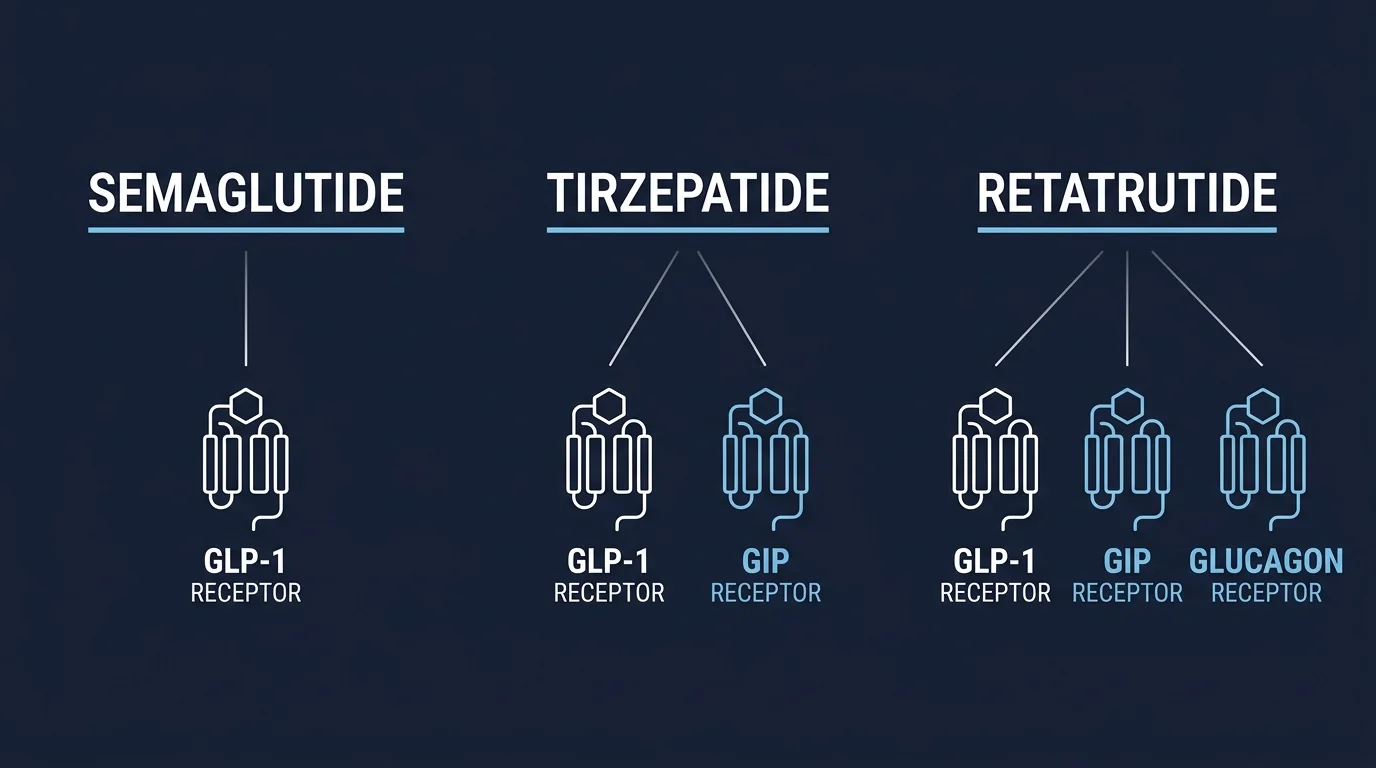
The clearest way to understand this class is by receptor. GLP-1 receptors, GIP receptors, and glucagon receptors each have distinct downstream signaling cascades. The three compounds hit those targets in different combinations.
Semaglutide is a GLP-1 receptor agonist. It shares roughly 94% sequence homology with native GLP-1(7-36) amide but carries a C-18 fatty diacid chain at lysine-34 that enables albumin binding, extending its half-life in serum from minutes (for native GLP-1) to approximately seven days in research models. It hits one receptor.
Tirzepatide is a dual GIP/GLP-1 agonist. A single synthetic peptide with affinity for both the glucose-dependent insulinotropic polypeptide receptor and the GLP-1 receptor. The GIP component was historically treated as a secondary target, but tirzepatide’s SURMOUNT program established GIP co-agonism as a meaningful contributor to the compound’s pharmacology. Two receptors, one molecule.
Retatrutide adds a third: glucagon receptor agonism. GLP-1 plus GIP plus glucagon. The glucagon component is what makes retatrutide mechanistically distinct from both predecessors. Glucagon receptor signaling in the liver affects hepatic glucose output and lipid oxidation pathways that GLP-1 agonism alone does not address. TRIUMPH-4 trial data, currently emerging from Eli Lilly’s Phase III program, is the primary clinical backdrop for researchers studying this compound in preclinical models.
Semaglutide: Research Profile and Sourcing Notes
Semaglutide has the most mature research supply chain of the three. It was the first of this class to reach widespread research-compound availability, and the testing infrastructure around it reflects that history. HPLC purity reports are standard across serious suppliers, though the quality of identity confirmation still varies.
Molecular weight is approximately 4,113 Da. The C-18 fatty diacid side chain that enables albumin binding also makes lyophilized storage the preferred shipping state. The molecule degrades faster in solution than the shorter-chain peptides in this class. Bacteriostatic water is the standard reconstitution diluent in research protocols; sterile water is a viable alternative but offers no antimicrobial protection across the working life of a reconstituted vial.
On the COA side: semaglutide is well-characterized enough that sequence errors in supply are relatively rare. Purity variation across vendors is not rare, though. Across the Match-Batch COAs we have reviewed, semaglutide lots cluster around 98-99% HPLC purity when properly sourced. Material that tests at 95-96% is a procurement red flag worth investigating before a lot enters any protocol. We consider semaglutide COAs without an LC-MS trace incomplete, even at this supply-maturity level, because the albumin-binding side chain is not visible in purity data alone.
Tirzepatide: Research Profile and Sourcing Notes
Tirzepatide is a 39-amino-acid synthetic peptide with a molecular weight around 4,813 Da. The dual-agonist structure makes it a larger, more complex molecule than semaglutide. More residues means more opportunity for sequence errors or truncated variants that share similar HPLC profiles but differ on mass spectrometry. Short version: HPLC purity alone is not sufficient for tirzepatide identity confirmation.
This is a compound where we consider LC-MS identity confirmation non-negotiable. A 99% HPLC result tells you the sample is mostly one thing. It does not confirm that thing is tirzepatide. Mass spectrometry verifies the molecular weight and fragmentation pattern, which confirms sequence fidelity. Any COA that lacks a mass spec trace on tirzepatide is incomplete for serious research procurement.
Supply of tirzepatide as a research compound has stabilized through 2025-2026 after initial tightness that followed compounding pharmacy restrictions. Bastion supplies tirzepatide 5mg vials with full Match-Batch Janoshik documentation, including LC-MS identity verification on each lot.
Retatrutide: Research Profile and Sourcing Notes
Retatrutide is the newest of the three in research-compound availability. Triple-agonist peptides are structurally the most complex in this class, and supply maturity has not yet caught up to what exists for semaglutide. Molecular weight is approximately 4,811 Da, close to tirzepatide, but the sequence and glucagon-agonist pharmacophore are distinct.
The glucagon receptor component is the variable of primary research interest here. Glucagon’s hepatic effects on glycogenolysis and gluconeogenesis, and its role in adipose tissue lipid mobilization, are mechanistically separate from what GLP-1 agonism achieves. Researchers studying hepatic glucose output or energy expenditure pathways will find retatrutide is the only compound in this class that directly addresses the glucagon receptor in that context.
COA scrutiny matters more on retatrutide than on the other two. In our sourcing experience, identity-testing gaps are more common with this compound than with semaglutide or tirzepatide, because fewer labs have accumulated testing history on the molecule and vendor supply chains are less seasoned. Demand per-batch COA documentation before committing to a lot. Bastion’s retatrutide 5mg vials follow the same per-batch Janoshik standard applied across our full catalog.
COA Standards: What to Require Across All Three
All three are synthetic peptides, which means COA requirements share the same structure but differ in criticality by compound complexity.
| Compound | MW (approx.) | Receptors Targeted | Min. HPLC Purity | LC-MS Identity Required | Supply Maturity (2026) |
|---|---|---|---|---|---|
| Semaglutide | ~4,113 Da | GLP-1 | ≥98% | Yes | High |
| Tirzepatide | ~4,813 Da | GLP-1 + GIP | ≥98% | Yes (critical) | Moderate-High |
| Retatrutide | ~4,811 Da | GLP-1 + GIP + Glucagon | ≥98% | Yes (critical) | Moderate |
The “critical” notation for tirzepatide and retatrutide reflects their structural complexity. A 99% HPLC result on a large synthetic peptide with possible truncated variants is not reassuring without mass spec confirmation. We have seen batches from non-Match-Batch suppliers that returned high HPLC purity but showed identity discrepancies on LC-MS review. Per-batch third-party testing exists precisely to catch that failure mode before it enters a study design.
Reconstitution Considerations for Research Use
All three compounds ship as lyophilized powder and require reconstitution before use in solution-phase research. The practical difference is in concentration math. Working concentrations vary across the three depending on the study design, and the margin for reconstitution error scales with molecular weight. Semaglutide at 4,113 Da and the two near-4,800 Da compounds are not interchangeable in dilution calculations even if the vial mass is identical.
Standard diluent is bacteriostatic water. Inject the water slowly against the vial wall rather than directly onto the lyophilized cake, and avoid agitation. These are large, structurally sensitive peptides. After reconstitution, refrigerate at 2-8°C, protect from light, and avoid repeated freeze-thaw cycles across all three compounds.
For the concentration and volume calculations, InjectBuddy’s peptide reconstitution calculator is a free browser-based tool that handles dilution math for these compounds without requiring any software. Practical for research groups managing multiple compounds with different working concentrations across the same experimental cycle.
Selecting the Right Compound for a Research Protocol

The choice is mechanism-driven, not potency-driven. These are not interchangeable compounds at different dose levels. They hit different receptor combinations, and the downstream signaling cascades they activate overlap but are not identical.
GLP-1-receptor-only research: semaglutide is the cleanest tool. The monoagonist profile isolates GLP-1R signaling without GIP or glucagon confound.
Dual GLP-1/GIP signaling studies: tirzepatide. The GIP component is the variable of interest, not a side effect of the formulation.
Triple-receptor or glucagon-pathway studies: retatrutide. It is the only compound in this class with meaningful glucagon receptor agonism alongside GLP-1 and GIP.
Research groups running cross-compound comparisons should source from the same vendor, in the same batch cycle, with COAs from the same testing lab. Cross-vendor comparisons introduce compound-quality variance as an uncontrolled variable. Bastion’s research affiliate program provides procurement documentation access for institutional and review-team purposes.
Frequently Asked Questions
What is the main difference between semaglutide, tirzepatide, and retatrutide?
The receptor targets. Semaglutide is a GLP-1 monoagonist. Tirzepatide adds GIP receptor agonism to GLP-1. Retatrutide adds a third receptor, glucagon, to the GLP-1 and GIP targets tirzepatide already hits. The three represent successive additions to the receptor target profile, not dose escalations of the same compound.
Is retatrutide available as a research compound in 2026?
Yes, though supply maturity is lower than for semaglutide or tirzepatide. Retatrutide became available as a research compound as the TRIUMPH-4 trial progressed and manufacturing interest followed clinical attention. COA documentation standards are less consistent across suppliers for retatrutide than for the older two compounds, which makes per-batch verification more important, not less.
What COA should I require when sourcing tirzepatide or retatrutide?
At minimum: HPLC purity ≥98% plus LC-MS identity confirmation on the specific lot you are receiving. Mass spectrometry is non-negotiable for these larger synthetic peptides because truncated variants can produce misleadingly high HPLC purity numbers while failing identity verification. The COA should resolve to a verifiable record on the testing lab’s own database, not a vendor-hosted PDF.
How do I reconstitute semaglutide, tirzepatide, or retatrutide for research use?
All three ship lyophilized and are reconstituted with bacteriostatic water. Inject diluent slowly against the vial wall, avoid agitation, and do not shake. Working concentration depends on the vial mass and diluent volume. Because the three compounds differ in molecular weight, the same vial mass produces different molar concentrations at the same diluent volume. InjectBuddy’s peptide reconstitution calculator handles this math in a browser at no cost.
Does semaglutide require different storage conditions than tirzepatide or retatrutide?
All three are stored similarly in lyophilized form: cold, dry, protected from light. The C-18 fatty diacid chain on semaglutide makes its reconstituted form slightly more sensitive to temperature fluctuation, but the practical handling guidance is similar across all three: refrigerate reconstituted material at 2-8°C, limit freeze-thaw cycles, and use within the window supported by the lot’s stability data.
Why does the glucagon receptor component in retatrutide matter for research?
Glucagon receptor signaling has distinct hepatic effects including stimulation of glycogenolysis and influence over gluconeogenesis that GLP-1 receptor agonism alone does not replicate. For researchers studying hepatic glucose metabolism, lipid oxidation, or energy expenditure pathways, the glucagon component in retatrutide is the variable that separates it from tirzepatide. It is not a stronger version of tirzepatide; it is a compound with a third mechanistic arm.
Can I source all three compounds from the same vendor?
Yes, and for comparative research this is the preferred approach. Single-vendor sourcing with consistent per-batch COA documentation reduces compound quality as an uncontrolled variable in cross-compound study designs. Bastion supplies all three as Janoshik Match-Batch-verified, lyophilized vials with US and Canada fulfillment and free re-ship on customs seizures.
What is the TRIUMPH-4 trial and why does it matter for retatrutide research context?
TRIUMPH-4 is Eli Lilly’s Phase III trial program for retatrutide as an investigational therapeutic. It provides the clinical backdrop researchers reference when contextualizing preclinical retatrutide work. The primary question the trial addresses is whether glucagon receptor co-agonism adds meaningful incremental pharmacology beyond what the GLP-1/GIP combination in tirzepatide achieves. Preclinical literature on this question predates the trial, but TRIUMPH-4 data is the most current clinical reference point available.
Conclusion
Semaglutide, tirzepatide, and retatrutide are not competing versions of the same compound at different potencies. They target different receptor combinations and answer different research questions. The selection between them is mechanism-driven: GLP-1 only, GLP-1 plus GIP, or all three plus glucagon.
On the procurement side, COA rigor scales with structural complexity. Semaglutide’s supply chain is the most mature. Tirzepatide and retatrutide demand LC-MS identity confirmation on every sourced lot because their molecular complexity creates supply-error modes that HPLC purity alone will not detect. All three are available as Janoshik Match-Batch-verified compounds through Bastion, with free re-ship to the US and Canada.
Research Use Only. Not for human consumption. The information above is provided for in-vitro and laboratory research context only and does not constitute medical advice, clinical guidance, or a recommendation for any form of human or veterinary use.