Research-use-only (RUO) notice. This article is an educational reference monograph intended for laboratory and research professionals. It is not medical advice, not a dosing guide, and not a statement of safety or efficacy in humans or animals. The peptide discussed is supplied and described strictly for in-vitro and laboratory research use only. Nothing here should be read as encouraging human or veterinary administration, diagnosis, treatment, or any clinical application. References to “activity,” “signalling,” or “effects” describe observations reported in cell-culture and animal-model literature, not therapeutic outcomes. Anyone handling research peptides is responsible for compliance with their own institutional, local, and national regulations governing the acquisition, storage, and use of research chemicals.
What KPV Is

KPV is a tripeptide composed of three amino acid residues in sequence: lysine (K), proline (P), and valine (V). It corresponds to the C-terminal fragment of alpha-melanocyte-stimulating hormone (α-MSH), specifically residues 11 through 13 of that thirteen-residue parent hormone. In other words, KPV is the tail end of α-MSH isolated as a standalone molecule. Its molecular simplicity is the entire reason it became a subject of research interest. It’s one of the shortest peptide sequences reported to retain a measurable portion of the anti-inflammatory signalling associated with the much larger parent hormone.
The significance of the fragment lies in what it leaves behind. Full-length α-MSH is a melanocortin agonist; among its documented actions is stimulation of melanogenesis, the pigment-producing pathway responsible for tanning of the skin. That pigmentary activity depends on the core melanocortin-receptor-binding motif located elsewhere in the α-MSH sequence. KPV lacks the residues required for high-affinity binding to the classical melanocortin receptors, and correspondingly it does not carry the pigmentary activity of the whole hormone. Researchers studying inflammation therefore became interested in KPV as a way to interrogate the anti-inflammatory arm of melanocortin biology while stripping away the pigment-driving function. This separation of activities, keeping the inflammation-related signalling while discarding the tanning effect, is the conceptual reason the fragment is studied at all.
Because it’s only three residues long, KPV is also a useful tool molecule. Small peptides are easier to synthesise to high purity. They’re easier to characterise analytically. And they raise different questions about cellular uptake and stability than large proteins do. That combination of biological interest and analytical tractability is why KPV recurs across several distinct research literatures rather than being confined to a single niche.
Mechanism and Pharmacology in Research Models
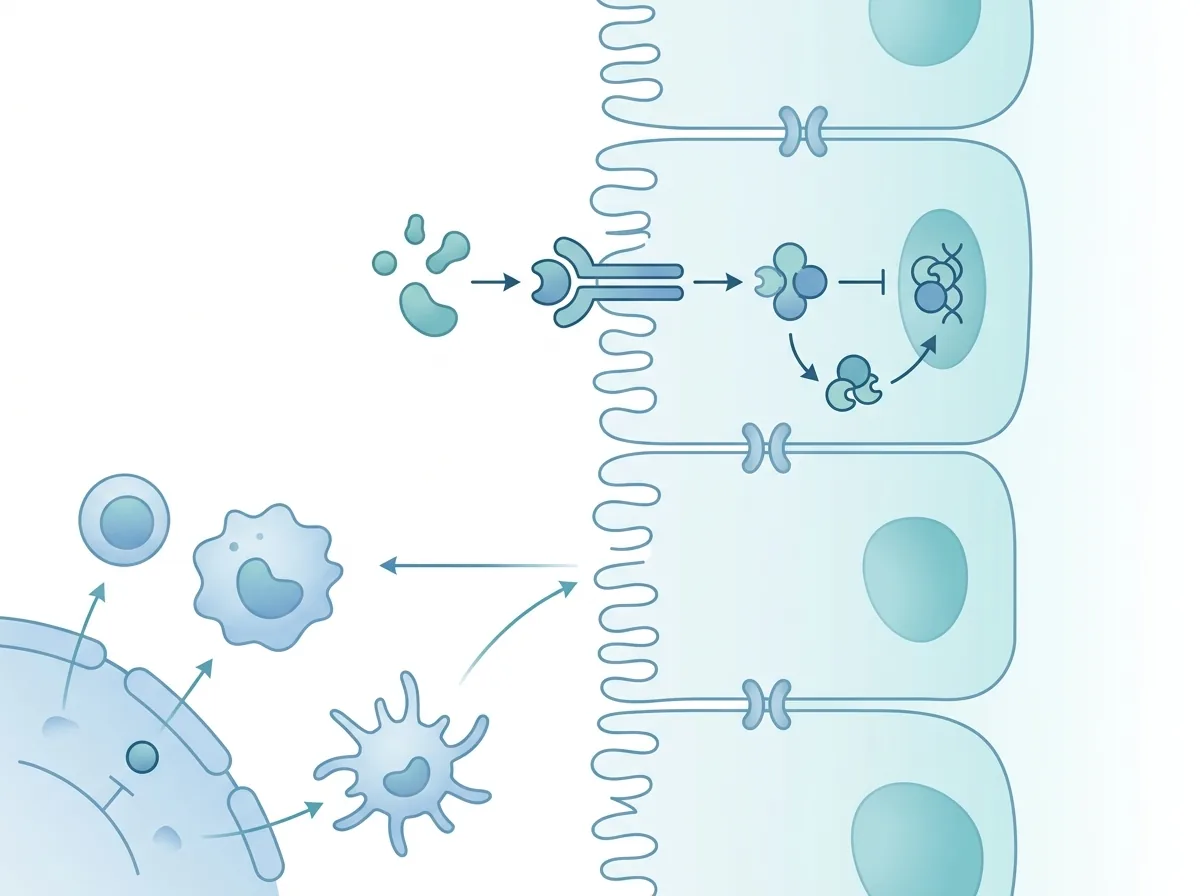
The dominant theme in the KPV literature is dampening of pro-inflammatory signalling. In cell-culture systems, KPV has been reported to reduce the activation of the nuclear factor kappa-B (NF-κB) pathway, a central transcriptional control point that governs the expression of many inflammatory mediators. The NF-κB pathway is normally held inactive in the cytoplasm by inhibitory IκB proteins; upon a pro-inflammatory stimulus, IκB is phosphorylated and degraded, freeing NF-κB to translocate into the nucleus and switch on inflammatory gene programs. Research on KPV describes interference with this cascade. The observations are consistent with reduced NF-κB nuclear translocation and reduced downstream transcription of pro-inflammatory cytokines in the model systems studied.
A noteworthy feature of the reported mechanism is that it appears, in several studies, to operate without requiring engagement of the cell-surface melanocortin receptors that mediate α-MSH’s pigmentary and some of its other classical effects. This is mechanistically interesting because it implies that at least part of KPV’s anti-inflammatory signalling in these models is receptor-independent at the membrane and instead involves the peptide acting on intracellular targets. That, in turn, raises the question of how a charged tripeptide reaches the cytoplasm at all.
This is where cellular uptake becomes a research topic in its own right. Several studies have examined whether and how KPV is internalised by cells, with particular attention to epithelial systems such as intestinal epithelial cells. Work in this area has explored the possibility that KPV is taken up via peptide-transport machinery present on epithelial cells rather than by passive diffusion, which would fit its small size and the observation of intracellular activity. The practical research consequence is that KPV is frequently studied in epithelial and barrier-tissue contexts where such transporters are expressed and where its anti-inflammatory readouts can be measured directly.
Frame all of the above as mechanism described in laboratory models. The pathways named (NF-κB, IκB, cytokine transcription) are well-characterised biology. But the magnitude, durability, and physiological relevance of KPV’s reported effects are properties of specific experimental systems, not established human pharmacology.
What the Research Investigates
KPV appears across a handful of recurring research areas. The most prominent is intestinal inflammation. Experimental models of colitis, whether chemically induced or otherwise, have been used to ask whether KPV reduces markers of mucosal inflammation, attenuates pro-inflammatory cytokine signalling in gut epithelial tissue, or influences epithelial barrier behaviour. The epithelial-uptake findings described above dovetail with this line of work, because intestinal epithelial cells are a natural site to study a small peptide that may be transported into cells and act on inflammatory signalling there.
A second area is epithelial and wound-associated inflammation more broadly. Beyond the gut, researchers have examined KPV in skin keratinocyte systems and other epithelial models, partly because of the α-MSH lineage (α-MSH biology is heavily studied in skin) and partly to probe the same anti-inflammatory readouts in a different tissue context. In these models the questions tend to center on cytokine output and inflammatory-pathway activation in response to stimuli.
A third area is antimicrobial-peptide research. KPV and closely related α-MSH-derived fragments have been studied for reported activity against certain microorganisms in laboratory assays, situating them within the broader field of host-defence and antimicrobial peptides. This is a distinct research question from the anti-inflammatory work and should not be conflated with it.
Across these areas, a unifying theme is the “resolution of inflammation” framing. Rather than being studied as a broad immunosuppressant, KPV is typically investigated as a molecule that modulates specific inflammatory signalling nodes in defined cell and tissue systems. The following list summarises the principal reported research contexts:
- Intestinal-inflammation models: experimental colitis and gut epithelial systems, with attention to mucosal inflammatory markers and epithelial uptake.
- Epithelial and wound-inflammation models: keratinocyte and other epithelial systems examining cytokine and pathway-level readouts.
- Antimicrobial-peptide research: laboratory assays of activity against microorganisms, within host-defence peptide studies.
- Resolution-of-inflammation studies: cell and tissue systems probing modulation of NF-κB-associated signalling and downstream cytokines.
KPV Compared With Related Peptides
The most direct comparison is to KPV’s own parent, full-length α-MSH. The two share an anti-inflammatory research profile, but they differ in two decisive ways. First, α-MSH carries pigmentary (melanogenic) activity through its melanocortin-receptor-binding core, while KPV does not. Second, α-MSH is a larger peptide with broader receptor engagement, whereas KPV is the minimal C-terminal fragment studied specifically to isolate anti-inflammatory signalling from the rest of the hormone’s pharmacology. So KPV is best understood not as a substitute for α-MSH but as a reductionist research tool for one slice of α-MSH biology.
KPV is also frequently mentioned alongside other research peptides studied in tissue-repair and anti-inflammatory contexts, most notably BPC-157 and TB-500 (a thymosin beta-4 fragment). Be precise here. These are entirely different molecules with different sequences, origins, and proposed mechanisms. BPC-157 is a synthetic peptide derived from a gastric protein sequence and is studied in connective-tissue and gastrointestinal repair models. TB-500 relates to actin-binding thymosin beta-4 biology. They overlap with KPV only in that all three appear in research literatures concerned with inflammation, healing, and tissue integrity. They do not share KPV’s α-MSH lineage or its specific NF-κB-associated mechanism, and grouping them reflects a shared research theme rather than mechanistic equivalence. Readers comparing these molecules can review the dedicated BPC-157 and TB-500 research guide and the broader longevity research peptides guide for how each is positioned in the literature.
What the Literature Does NOT Establish
Sober interpretation requires being explicit about the boundaries of the evidence. The KPV research base is predominantly cell-culture and animal-model work. That distinction carries real weight, and several limitations follow directly from it.
- Model-system results are not human outcomes. Anti-inflammatory readouts in colitis models or epithelial cell lines do not establish that KPV is safe, effective, or appropriate for any human or veterinary use. The translational gap between such models and clinical reality is large and is not bridged by the existing literature.
- There is no established human dose, regimen, or route. Because this is research-use-only material, no dosing information is provided or implied. Any figure presented elsewhere as a “dose” is not supported by the kind of controlled human evidence that would justify it.
- Mechanistic findings are model-specific. Reported NF-κB-associated effects and uptake behaviour were observed in particular systems; their magnitude and relevance can differ between cell types and conditions and should not be generalised.
- Long-term safety, pharmacokinetics, and interactions in intact organisms are not characterised to the standard that clinical decisions would require.
- Antimicrobial and anti-inflammatory observations are distinct and should not be merged into a single overstated profile.
In short, KPV is an interesting research molecule with a coherent and reproducible set of laboratory observations behind it, and simultaneously a substance whose therapeutic value in humans is unestablished. Both statements are true at once, and responsible research framing holds them together.
Handling, Reconstitution, and Stability
Research peptides such as KPV are typically supplied as a lyophilised (freeze-dried) powder under vacuum or inert atmosphere. In dry, lyophilised form the peptide is comparatively stable and tolerant of short ambient exposure during shipping, but it should be moved to appropriate cold storage on receipt. For longer-term storage of the unreconstituted powder, cold and dark conditions are standard practice; freezer storage is generally preferred for extended periods, and exposure to heat, humidity, and light should be minimised throughout.
For laboratory reconstitution, bacteriostatic water is the conventional diluent for multi-use research solutions because the benzyl alcohol it contains suppresses microbial growth across repeated vial entries; sterile or sterile-filtered water may be used where a single-use, additive-free solution is required by the protocol. The diluent should be introduced gently down the vial wall rather than injected forcefully onto the peptide cake, and the vial should be swirled rather than shaken vigorously, since mechanical shear and foaming can degrade peptides. Once in solution, KPV is markedly less stable than the dry powder and should be kept refrigerated and protected from light.
For research workflows that involve repeated sampling, preparing single-use aliquots and freezing them avoids subjecting the whole stock to repeated freeze-thaw cycles, each of which can contribute to degradation. Concentration planning means matching the mass of peptide per vial to the diluent volume needed for a target working concentration. That’s where most handling errors occur. The peptide reconstitution calculator guide walks through that arithmetic so that volumes and concentrations are derived rather than guessed.
Verifying Purity and Identity
For a research peptide, analytical verification isn’t optional housekeeping. It’s the foundation of whether any downstream result can be trusted. Two things matter: that the vial contains the molecule it claims to (identity) and that it’s sufficiently free of synthesis-related impurities (purity). The standard tools are high-performance liquid chromatography (HPLC) for purity quantification and mass spectrometry for identity confirmation against the expected molecular mass of the lysine-proline-valine sequence.
The most credible evidence is independent, third-party testing reported on a per-lot basis. A certificate of analysis (COA) that corresponds to the specific batch in hand, rather than a generic or representative document, lets a researcher tie observed results to a characterised material. Bastion publishes batch testing through its lab results library and operates a Janoshik match-batch process so that the report can be matched to the lot received. Reading these reports is a skill in itself. You need to know what the chromatogram peaks, the reported purity percentage, and the mass data actually tell you. The guide to reading a peptide COA provides a walkthrough of how to interpret a Janoshik report rather than taking a headline number at face value.
Frequently Asked Questions
Is KPV the same thing as α-MSH?
No. KPV is the C-terminal three-residue fragment of α-MSH (residues 11–13). It’s a distinct, much smaller molecule that retains part of the anti-inflammatory signalling associated with α-MSH in research models but lacks the melanocortin-receptor-binding region responsible for the parent hormone’s pigmentary (tanning) activity.
Why is KPV studied instead of just using α-MSH?
Researchers use KPV precisely because it separates functions. By isolating the C-terminal fragment, studies can probe α-MSH’s anti-inflammatory arm without the confounding pigmentary effects of the full hormone, and they gain a small, analytically tractable molecule whose cellular uptake and intracellular activity can be examined directly.
What does KPV do at the molecular level in research models?
In cell-culture and animal-model studies, KPV is reported to dampen pro-inflammatory signalling associated with the NF-κB pathway and its downstream cytokines, in several cases apparently without requiring cell-surface melanocortin receptors. Research has also examined how the peptide is taken up into epithelial cells. These are model-system observations, not established human pharmacology.
How is KPV related to BPC-157 or TB-500?
Only thematically. All three appear in research literatures concerned with inflammation and tissue repair, but they are chemically unrelated molecules with different origins and proposed mechanisms. KPV’s α-MSH lineage and NF-κB-associated signalling are not shared by BPC-157 or TB-500, so they should not be treated as interchangeable.
How should KPV be stored in a research setting?
As a lyophilised powder it’s kept cold and dark, with freezer storage preferred for long-term holding. Once reconstituted, typically with bacteriostatic water for multi-use solutions, it’s less stable and should be refrigerated, protected from light, and ideally aliquoted to avoid repeated freeze-thaw cycles.
Summary
KPV is a lysine-proline-valine tripeptide corresponding to the C-terminal fragment (residues 11–13) of α-melanocyte-stimulating hormone. Its research interest stems from being a minimal fragment that retains part of α-MSH’s anti-inflammatory signalling, including effects associated with the NF-κB pathway and downstream cytokines, while shedding the pigmentary activity of the full hormone. Because it is small, it has also become a subject for studies of cellular uptake in epithelial systems and for work spanning intestinal-inflammation models, epithelial and wound-inflammation models, and antimicrobial-peptide research. Set against this is a clear and unbridged limitation: the evidence is overwhelmingly preclinical, no human dose or therapeutic claim is established, and model-system findings do not translate into clinical conclusions. For research use, the practical priorities are correct handling and storage of the lyophilised material, careful reconstitution, and above all per-lot analytical verification of purity and identity through independent HPLC and mass spectrometry so that any experimental result rests on a characterised, traceable material.